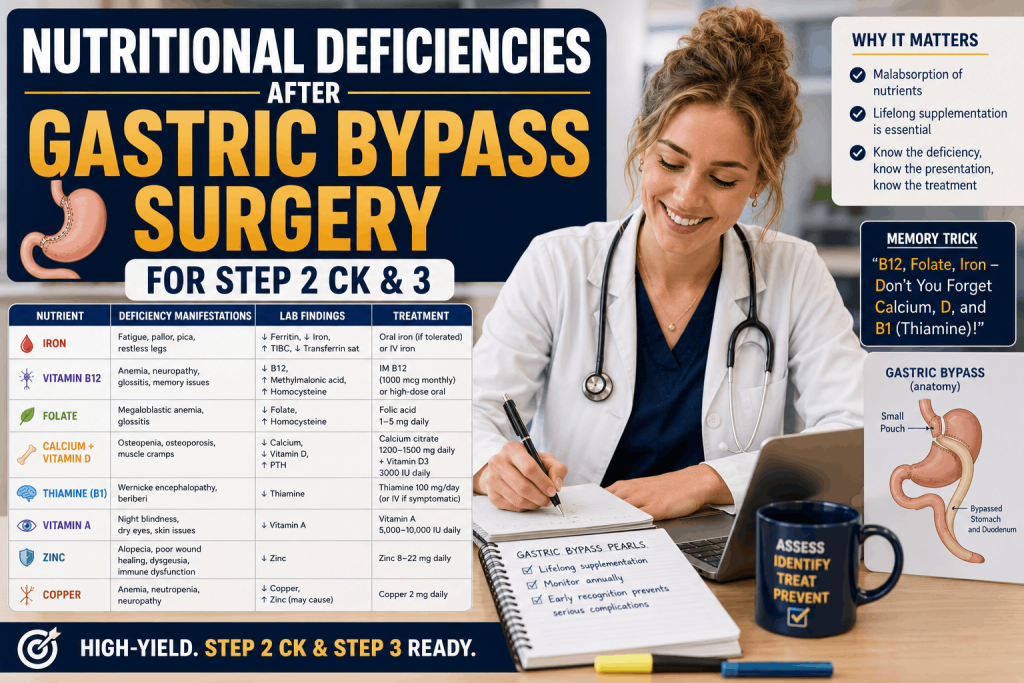

Nutritional Deficiencies After Gastric Bypass Surgery is a high-yield Step 2 CK and Step 3 topic because exam questions often present a patient months or years after bariatric surgery with anemia, neuropathy, confusion, bone pain, weakness, or abnormal labs.
Students struggle with this topic because they try to memorize a long vitamin list without connecting the deficiency to the surgery, the anatomy, the timeline, and the clinical presentation.
The clinical reasoning solution is simple: gastric bypass changes nutrient intake, stomach acid exposure, intrinsic factor physiology, duodenal absorption, and fat-soluble vitamin absorption. Once you understand that mechanism, the answer choices become much easier.
This guide will break down the most important gastric bypass nutritional deficiencies for Step 2 CK and Step 3, including thiamine, vitamin B12, iron, calcium, vitamin D, folate, copper, zinc, protein, and fat-soluble vitamins.
Free USMLE Training
Free USMLE Step 1 Bootcamp
Join our free USMLE masterclass to learn high-yield clinical reasoning systems for nutrition, internal medicine, surgery, and test-day decision-making.
Reserve My SpotNutritional Deficiencies After Gastric Bypass Surgery
On Step 2 CK and Step 3, gastric bypass deficiency questions are usually not written as simple recall questions. They are written as clinical vignettes.
The patient may present with:
- Vomiting and confusion after bariatric surgery.
- Macrocytic anemia and neuropathy.
- Microcytic anemia and fatigue.
- Bone pain, fractures, or secondary hyperparathyroidism.
- Ataxia, ophthalmoplegia, or memory changes.
- Posterior column findings that look like B12 deficiency but are actually copper deficiency.
The Big Rule
If a post-bariatric surgery patient has neurologic symptoms, always think about thiamine, B12, and copper before choosing a simple explanation like dehydration or anxiety.
Why Gastric Bypass Causes Deficiencies
Roux-en-Y gastric bypass reduces stomach size and bypasses the duodenum and proximal jejunum. That matters because many nutrients depend on stomach acid, intrinsic factor, or proximal small bowel absorption.
This is why the highest-yield deficiencies include iron, vitamin B12, calcium, vitamin D, folate, thiamine, copper, and fat-soluble vitamins.
| Mechanism | Deficiency Risk | USMLE Clue |
|---|---|---|
| Reduced intake | Protein, thiamine, folate | Poor intake, vomiting, rapid weight loss |
| Reduced acid exposure | Iron, B12 | Anemia after surgery |
| Reduced intrinsic factor physiology | Vitamin B12 | Macrocytosis, neuropathy |
| Bypassed duodenum | Iron, calcium, copper | Microcytic anemia, bone disease, myelopathy |
| Fat malabsorption | Vitamins A, D, E, K | Night blindness, bone pain, neuropathy, bleeding |
Step 2 CK & Step 3 Study System
Step 2 CK & 3 Masterclass With AI and Self-Paced Course
If nutrition, surgery, internal medicine, and management questions feel overwhelming, the Step 2 CK & Step 3 Masterclass with AI and self-paced course can help you organize clinical reasoning and apply high-yield concepts to vignettes.
Explore Step 2 CK & Step 3 Course
High-Yield Deficiency Table
| Deficiency | Classic Presentation | Step 2 CK / Step 3 Clue |
|---|---|---|
| Thiamine B1 | Wernicke encephalopathy, neuropathy, beriberi | Vomiting after bariatric surgery plus confusion, ataxia, ophthalmoplegia |
| Vitamin B12 | Megaloblastic anemia, neuropathy, posterior column dysfunction | Macrocytosis, paresthesias, impaired vibration sense |
| Iron | Microcytic anemia, fatigue, pica | Low ferritin after bypass |
| Calcium / Vitamin D | Bone pain, osteomalacia, secondary hyperparathyroidism | Low vitamin D, high PTH, low or normal calcium |
| Folate | Megaloblastic anemia without neurologic deficits | Macrocytosis with poor intake |
| Copper | Myelopathy, neuropathy, anemia, neutropenia | B12-like symptoms with normal B12 |
| Vitamin A | Night blindness, dry eyes | Fat malabsorption clue |
| Vitamin K | Bleeding tendency | Elevated PT/INR |
High-Yield Nutrition Resource
Get the High Yield USMLE Nutrition Recall Book
This book covers high-yield USMLE nutrition topics like bariatric surgery deficiencies, vitamin deficiency presentations, malabsorption, anemia, neurologic clues, and nutrition-based clinical reasoning for Step 2 CK and Step 3.
Get the Nutrition Recall BookThiamine Deficiency After Gastric Bypass
Thiamine deficiency is one of the most dangerous deficiencies after gastric bypass because it can cause Wernicke encephalopathy.
The classic triad is:
- Confusion
- Ataxia
- Ophthalmoplegia
The Step 2 CK and Step 3 clue is a patient with recent bariatric surgery, persistent vomiting, poor intake, rapid weight loss, and neurologic symptoms.
Do Not Miss This
Treat suspected Wernicke encephalopathy with thiamine before giving glucose. On exams, this is a patient-safety management point.
Vitamin B12 and Iron Deficiency
Vitamin B12 Deficiency
Vitamin B12 deficiency after gastric bypass can occur because normal B12 absorption depends on gastric physiology, intrinsic factor, and terminal ileal absorption.
The exam clue is macrocytic anemia plus neurologic symptoms such as paresthesias, gait problems, or loss of vibration and proprioception.
Iron Deficiency
Iron deficiency is also high yield because iron is absorbed mainly in the duodenum and proximal jejunum, which are bypassed in Roux-en-Y gastric bypass.
The exam clue is microcytic anemia, low ferritin, fatigue, pica, or restless legs in a patient with prior bariatric surgery.
| Finding | Think | Why |
|---|---|---|
| Macrocytic anemia + neuropathy | B12 deficiency | Neurologic signs distinguish it from folate |
| Macrocytic anemia without neuropathy | Folate deficiency | Poor intake or malabsorption |
| Microcytic anemia + low ferritin | Iron deficiency | Duodenal absorption is impaired |
Recommended Nutrition Book
High Yield USMLE Nutrition Recall Book
The High Yield USMLE Nutrition Recall Book is designed to help you master nutrition topics that show up in clinical vignettes, including gastric bypass deficiencies, anemia patterns, vitamin deficiency clues, malabsorption, and nutrition management.
- Covers high-yield bariatric surgery deficiencies
- Connects nutrition facts to clinical presentations
- Useful for Step 2 CK, Step 3, COMLEX, and rotations
- Helps you recognize anemia, neurologic, and bone disease clues
Calcium and Vitamin D Deficiency
Calcium and vitamin D deficiency after gastric bypass can lead to bone pain, osteomalacia, fractures, hypocalcemia, and secondary hyperparathyroidism.
On exams, look for:
- Bone pain after bariatric surgery
- Low vitamin D
- Elevated parathyroid hormone
- Low or low-normal calcium
- Elevated alkaline phosphatase in osteomalacia
Clinical Reasoning Tip
If calcium absorption drops, PTH rises to maintain serum calcium. That is why secondary hyperparathyroidism is a classic clue.
Copper, Folate, and Neurologic Clues
Copper Deficiency
Copper deficiency is a favorite “trick” topic because it can mimic vitamin B12 deficiency.
Patients may have gait instability, sensory ataxia, posterior column dysfunction, anemia, or neutropenia. If the vignette looks like B12 deficiency but B12 is normal, think copper.
Folate Deficiency
Folate deficiency causes megaloblastic anemia, but it does not cause the neurologic findings seen with B12 deficiency.
USMLE Distinction
B12 causes macrocytic anemia with neurologic symptoms. Folate causes macrocytic anemia without neurologic symptoms. Copper can mimic B12 but may also include neutropenia.
Fat-Soluble Vitamin Deficiencies
Fat-soluble vitamin deficiencies are especially important when malabsorption is present.
| Vitamin | Deficiency Clue | USMLE Association |
|---|---|---|
| Vitamin A | Night blindness, xerophthalmia | Vision changes after malabsorption |
| Vitamin D | Bone pain, osteomalacia | Low vitamin D, high PTH |
| Vitamin E | Neuropathy, ataxia, hemolysis | Neurologic symptoms with fat malabsorption |
| Vitamin K | Bleeding, elevated PT/INR | Coagulation abnormality |
Step 2 CK and Step 3 Strategy
For Step 2 CK and Step 3, the key is not just knowing the deficiency. It is knowing what to do next.
How to Answer These Questions
- First, identify the surgery history.
- Next, identify the timeline and symptom pattern.
- Then connect the symptom to the nutrient deficiency.
- Finally, choose the safest next step in management.
| Vignette Clue | Likely Answer |
|---|---|
| Vomiting + confusion + ataxia after bypass | Thiamine deficiency |
| Macrocytosis + paresthesias | Vitamin B12 deficiency |
| Microcytosis + low ferritin | Iron deficiency |
| Bone pain + high PTH | Vitamin D / calcium deficiency |
| B12-like myelopathy + neutropenia | Copper deficiency |
Student Success Story
⭐ 4.8 Google Rating | 120+ ReviewsSee How Dr. Wilner Passed Step 1
Dr. Wilner’s story shows how structured preparation, disciplined review, and the right support system can help students move forward with confidence.
Want to learn the same clinical reasoning system used by SmashUSMLE students?
Join Free BootcampNeed Help Mastering Nutrition for Step 2 CK and Step 3?
The Step 2 CK & Step 3 Masterclass with AI and self-paced course can help you turn nutrition, surgery, medicine, and management topics into organized clinical reasoning patterns.
FAQ: Nutritional Deficiencies After Gastric Bypass Surgery
What are the most common nutritional deficiencies after gastric bypass surgery?
The most common high-yield deficiencies include thiamine, vitamin B12, iron, calcium, vitamin D, folate, copper, zinc, protein, and fat-soluble vitamins A, D, E, and K.
Why is thiamine deficiency dangerous after gastric bypass?
Thiamine deficiency can cause Wernicke encephalopathy, especially in patients with persistent vomiting, poor intake, rapid weight loss, confusion, ataxia, or ophthalmoplegia.
What deficiency causes macrocytic anemia and neuropathy after gastric bypass?
Vitamin B12 deficiency causes macrocytic anemia and neurologic symptoms such as paresthesias, gait problems, and impaired vibration or proprioception.
What deficiency causes microcytic anemia after gastric bypass?
Iron deficiency is the classic cause of microcytic anemia after gastric bypass because iron absorption depends heavily on the duodenum and proximal jejunum.
How should I study nutritional deficiencies after gastric bypass surgery for Step 2 CK and Step 3?
Study each deficiency by pairing the surgery mechanism with the clinical clue. For example, vomiting plus confusion suggests thiamine deficiency, while macrocytosis plus neuropathy suggests B12 deficiency.
Ready to Improve Your USMLE Scores?
Nutrition questions become easier when you connect mechanisms to clinical vignettes. Join SmashUSMLE for free training, structured courses, tutoring, and the High Yield USMLE Nutrition Recall Book.